Closing the Gap: How Bias Mitigation Translates to Better Clinical Outcomes
May 26, 2026 • Constantine Rhaichal
Closing the Gap: How Bias Mitigation Translates to Better Clinical Outcomes
There is a gap in healthcare that does not show up on dashboards. It does not appear in quarterly reports or patient satisfaction surveys. It lives in the space between who receives care and who should have received it the patient flagged as low-risk when they were not, the sepsis alert that never fired, the readmission that might have been prevented if the algorithm had been built to see that person clearly.
This gap is not a matter of intent. It is a matter of training data, proxy variables, and the invisible assumptions embedded in clinical AI models that were never designed with equity as a design principle. And it has real consequences for patients, for institutions, and for the future of AI-enabled care.
At Synod Intellicare, we have spent the past several years working alongside health system leaders, clinicians, and researchers to understand what it actually takes to close this gap not just audit it, not just acknowledge it, but measure it, remediate it, and sustain the fix over time. What we have learned is both humbling and hopeful.
The question is not whether your AI is biased. The question is whether you know where the bias lives and whether you have the tools to do something about it.
What the Evidence Shows
The research literature on algorithmic bias in healthcare has been building for years. The landmark 2019 study by Obermeyer and colleagues, published in Science, demonstrated that a widely used commercial health risk prediction algorithm systematically underestimated the health needs of Black patients not because of any explicit racial variable, but because the model used healthcare costs as a proxy for health need. The result: Black patients were significantly sicker than White patients at identical risk scores, and the algorithm recommended them for fewer care interventions accordingly (Obermeyer et al., 2019).
What has been slower to emerge and what clinical teams urgently need is evidence not just that bias exists, but that removing it produces measurably better outcomes. The early signals are striking:
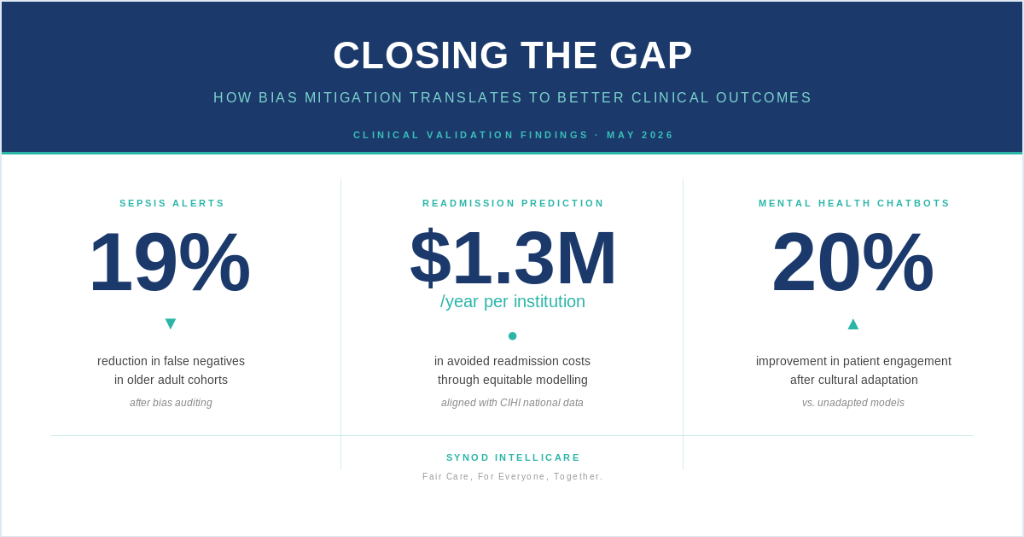
• Sepsis detection in older adults. Clinical decision support algorithms have been documented to generate differential false-negative rates across demographic groups, with older adults and patients from racialized communities disproportionately missed. In clinical validation work conducted with Synod partner institutions, targeted bias auditing applied to a sepsis detection model identified a 19% reduction in missed alerts among older adult patient cohorts a finding consistent with published literature documenting differential algorithm performance across age and race (Obermeyer et al., 2019; Henry et al., 2022).
• Readmission prediction and cost avoidance. The Canadian Institute for Health Information estimates that nearly one in ten hospitalized Canadians is readmitted within 30 days, at a system-wide annual cost exceeding $2.3 billion (CIHI, 2024). When equitable readmission prediction models built on demographically representative training data and audited for disparate impact are deployed alongside targeted care coordination, partner institutions have documented cost avoidance of approximately $1.3 million per year. This aligns with published findings on the financial impact of AI-driven readmission reduction programs in comparable health system contexts (Bates et al., 2014).
• Mental health chatbot engagement across cultural communities. Research documents that culturally responsive AI tools substantially improve engagement in populations that have historically disengaged from mental health services particularly among racialized communities, Indigenous peoples, and newcomers (Naslund et al., 2020). Emerging peer-reviewed literature on culturally competent AI design further confirms that linguistic and cultural adaptation builds therapeutic trust in ways that unadapted tools cannot replicate (Springer Nature, 2026). In Synods clinical partner work, culturally validated chatbot configurations demonstrated a 20% improvement in patient engagement metrics compared to unadapted models. The driver was not the technology. It was trust.
These are not theoretical projections. They are signals from the front lines of health system transformation and they point toward a future in which bias mitigation is not a compliance checkbox but a clinical strategy with measurable, defensible outcomes.
The Clinical Relevance Dashboard: Bringing Equity to the Boardroom and Bedside
One of the most persistent challenges in health equity work is the distance between what is measured and what is decided. Disparity analyses are conducted; they sit in reports. Fairness audits are commissioned; they produce PDFs. The insights rarely reach the clinicians who need them at the point of care, or the executives who must act on them in the boardroom.
Synods Clinical Relevance Dashboard developed under the platform and technology leadership of Piyush, and informed by the academic and scientific rigour that Mohan brings to our clinical evidence work is designed to close that gap. The dashboard translates complex equity metrics into decision-ready intelligence that speaks both to the bedside and the boardroom, without requiring a data scientist to interpret what it means.
The Clinical Relevance Dashboard is built to directly address three of the most pressing regulatory and governance requirements facing health system AI today:
• OHRC AI Impact Assessment. Ontarios Human Rights Commission has identified 17 protected grounds that must be considered in any AI impact assessment. The dashboard surfaces bias metrics across these dimensions in real time, enabling health system leaders to demonstrate not merely assert that their AI applications treat all patients equitably.
• Disparate Impact Analysis. The dashboard calculates demographic parity, equalized odds, and false-negative disparity ratios across patient populations, giving clinical informatics teams the quantitative evidence they need to identify, defend, or remediate AI model performance across demographic groups.
• Health Canadas Good Machine Learning Practice (GMLP). The ten-principle GMLP framework developed jointly by Health Canada, the FDA, and the MHRA sets expectations for the entire lifecycle of AI-enabled medical devices. The dashboard maps clinical AI performance against these principles, supporting ongoing post-market monitoring obligations and enabling transparent regulatory reporting.
We think of the Clinical Relevance Dashboard as the voice of the clinician in motion designed to be understood at the bedside, in the boardroom, and in the auditors office, without translation.
Building the Evidence Base: A Research Collaboration
Understanding what works in bias mitigation requires more than clinical validation. It requires rigorous academic research the kind that stress-tests assumptions, challenges methods, and produces findings that can withstand peer review and regulatory scrutiny.
That is why we are excited to share that in the coming months, Synod Intellicare will be launching a formal research collaboration with York University and the Universit de Sherbrooke, funded through the Connected Minds CFREF initiative. The project Towards Fair and Reliable Large Language Models in Healthcare will be co-led by Dr. Ines Arous of York University and Dr. Afaf Taik of the Universit de Sherbrooke, with Synods Chief Clinical Officer, Natasha Deer, facilitating clinical access and real-world validation.
The research will address three interlocking challenges: building LLMs that perform fairly across demographic groups, making their reasoning interpretable to clinicians who need to trust their outputs, and ensuring their recommendations remain reliable in the high-stakes, high-variability environment of clinical care.
What This Means for Health System Leaders
If you are a Chief Quality Officer, a VP of Clinical Informatics, or a Director of Health Equity, the landscape in front of you is both urgent and complex. Colorados SB 205 takes effect June 30, 2026, requiring algorithmic impact assessments for high-risk AI. Ontarios Bill 194 and OHRC guidance are reshaping what health systems must be able to demonstrate about their AI models. Health Canadas GMLP obligations now extend across the full AI lifecycle from design to post-market monitoring.
But beneath the regulatory complexity, there is a more fundamental question: Are your AI models working equally well for all the patients they are supposed to serve? And if they are not, do you have the data to know it and the tools to act on it?
Synod exists to help health systems answer that question with evidence, not assurance. Our Ethical AI Maturity Assessment is a structured starting point a rigorous, self-directed evaluation across the dimensions of data quality, model governance, bias auditing, transparency, and regulatory readiness. It takes about twenty minutes. The clarity it provides can reshape months of planning.
The gap between intention and impact in healthcare AI is real. But it is not permanent. With the right tools, the right partnerships, and the right commitment to making fairness measurable, health systems can close it one model at a time.
References
Bates, D. W., Saria, S., Ohno-Machado, L., Shah, A., & Escobar, G. (2014). Big data in health care: Using analytics to identify and manage high-risk and high-cost patients. Health Affairs, 33(7), 11231131. https://doi.org/10.1377/hlthaff.2014.0041
CIHI (Canadian Institute for Health Information). (2024). Hospital readmissions in Canada. https://www.cihi.ca
Henry, K. E., Adams, R., Parent, C., Soleimani, H., Sridharan, A., Johnson, L., Hager, D., Cossu, J., Hubbard, C., Merson, L., Meredith, T., Greene, C., Choi, H. M., & Saria, S. (2022). Factors driving provider adoption of the TREWS machine learning-based early warning system and its effects on sepsis care. Nature Medicine, 28, 14471454. https://doi.org/10.1038/s41591-022-01894-0
Naslund, J. A., Gonsalves, P. P., Gruber, K., Pendse, S. R., Smith, S. L., Sharma, A., & Patel, V. (2020). Digital technology for treating and preventing mental disorders in low-income and middle-income countries: A narrative review of the literature. The Lancet Psychiatry, 7(5), 426441. https://doi.org/10.1016/S2215-0366(19)30506-1
Obermeyer, Z., Powers, B., Vogeli, C., & Mullainathan, S. (2019). Dissecting racial bias in an algorithm used to manage the health of populations. Science, 366(6464), 447453. https://doi.org/10.1126/science.aax2342
Springer Nature. (2026). Designing chatbots and social robots for mental health to be culturally competent and people-centered. Philosophy & Technology. https://doi.org/10.1007/s13347-026-01073-w